The accelerating pandemic of diabetes is recognised as one of the most significant public health dilemmas of our time1. The personal,health and societal costs of the disease are enormous, with populations in many parts of
the developing world predicted to have a much increased and disproportionate burden of diabetes by the year 2040 2.
The micro and macro-vascular complications of type-2 diabetes and associated cardiovascular morbidity (and
mortality) have wide-ranging implications for public health 3, 4.
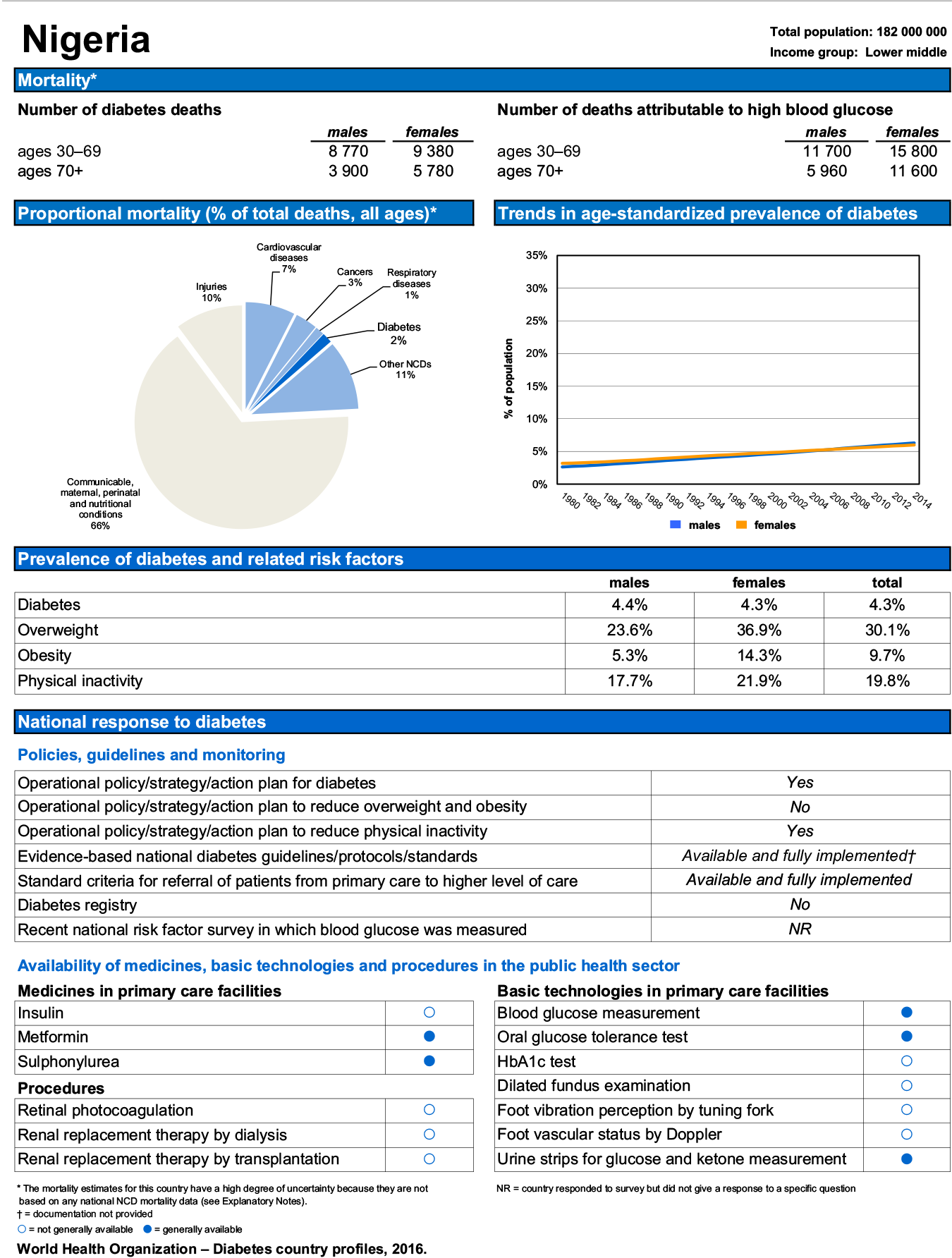
What do we know about the current and future burden of diabetes in Nigeria? The figures are largely unknown. The World Health Organization (WHO) estimates that approximately 5% of the country’s adult population is diabetic, 40% of which are either obese or overweight (fig 4).

Despite growing evidence that bariatric (metabolic) surgery offers a potentially costeffective treatment option for obese patients with type-2 diabetes, most established algorithms have until recently failed to fully recognise its benefits as a standard form of treatment for diabetes. This article explores the evolution of this treatment and the evidence underpinning its increasing use as a viable method of treating type-2 diabetes and associated metabolic conditions.
Types of Metabolic surgery
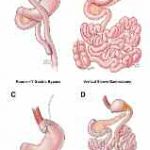
Bariatric (or Metabolic) surgery remains an exciting and rapidly advancing branch of gastrointestinal surgery with origins dating back to 19525. As one would expect, the surgical procedures performed have changed
significantly over the years. Fig 1 illustrates the four primary operations routinely performed in this field.
1. Roux-en-Y Gastric Bypass
2. Vertical Sleeve Gastrectomy
3. Laparoscopic Adjustable Gastric Banding
4. Biliopancreatic Diversion
Glucose homeostasis & GI surgery
The paradigm shift observed in the management of certain metabolic conditions is based entirely on emerging scientific evidence strongly suggesting that weight loss (or bariatric) surgery is capable of achieving resolution of long-term chronic diseases such as diabetes.
In 2007, an accumulation of these developments and increasing acceptance of the broader applicability of this form of surgical intervention resulted in the redefinition of the group of bariatric surgery procedures performed for the sole purpose of treating metabolic disease. Metabolic surgery was the term used to identify this group of surgical procedures.
The opportunity to conduct a series of complex operative procedures designed to rearrange the gastrointestinal anatomy and achieve enhancements in physiological and organ function offers many additional advantages to the management of chronic disease.
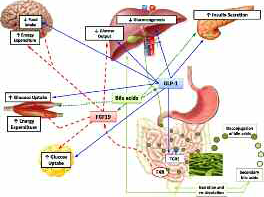
Corresponding improvements in glucose homeostatic control are associated with changes in gut hormones, bile acid metabolism and intestinal microbiomes. These result in the reduction of glucose production in the liver,
increased glucose utilisation in the tissues,increased insulin sensitivity and enhanced β-cell function, all of which occur independently, regardless of weight loss (fig 2).6
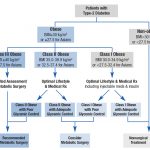
Bariatric surgery & type-2 diabetes guidelines
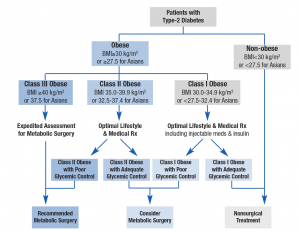
Although metabolic surgery is gaining rapid acceptance in treatment centres around the world, several obstacles to its universal uptake remain in existence in different regions. A series of consensus meetings held over the course of the last decade resulted in a series of agreed amendments to diabetes treatment guidelines now in use in various centres. In 2016, the 2nd Diabetes Surgical Summit (DSS 2) released the strongest ever endorsement of the procedure7.Metabolic surgery is now increasingly recommended as an established option (alongside lifestyle and medical treatment) in the management of obese patients with type-2 diabetes (fig 3). Studies have demonstrated
consistently better outcomes (specifically blood glucose and HbA1c control) in this group of patients compared with pharmacological treatment over the medium term (15 years or less). 8, 9,10,11,12,13
Setting up a service
There are several essential considerations in setting up a metabolic surgery service.
1. Multi-disciplinary team (MDT) approach – The MDT should consist of the following core specialists – bariatric surgeon, bariatric anaesthetist, an endocrinologist and bariatric dietitian. Other frequently involved specialists may include the cardiologist,respiratory physician, psychologist and physiotherapist.
2. Patient selection – Bariatric/metabolic surgery patients frequently have one or more chronic disease comorbidities. Careful selection, preparation and preoperative assessment of patients are critical to
ensuring good patient outcomes. Hospital infrastructure is also critical. Hospitals offering this service must be equipped to offer minimally-invasive and complex gastrointestinal surgery.
3. Outcome measures – It will be essential to measure (and monitor) service delivery outcomes by internationally-accepted evidence-based standards and treatment guidelines. Procedural outcome measures such as percentage excess weight loss (%EWL) and quality of life scoring may be applied to good effect. However, the most
reliable and straightforward parameters are as follows:
- Average post-operative length of stay (12-72 hours)
- Post-operative leak rate (3% or less)
- 30-day Operative mortality (0.4% or less)
 In conclusion
In conclusion
An increase in demand for bariatric and metabolic surgery services in Nigeria may be predicted by the combined effects of a rapidly increasing prevalence of type-2 diabetes and the overall state of evidence-based diabetes
care across the country. There is firm evidence to suggest the likelihood of significant benefit room this procedure especially in obese patients with type-2 diabetes and other forms of chronic metabolic disease.
The scale of future demand and capacity required for Nigeria’s healthcare system to meet that demand remains unknown.However, judging by the prevalence of diabetes-related comorbidity (and mortality), a substantial and coordinated response will be required to address this growing problem.
Metabolic surgery is gaining acceptance as an established component of diabetes guidelines all over the world. The main obstacles to delivery locally will be cost, and a shortage of appropriately trained clinical
personnel organised specialist facilities and support infrastructure.
Patients are likely to seek treatment abroad until the capacity and quality of healthcare services in Nigeria improve. As more specialist centres turn their attention towards innovative treatments such as metabolic surgery, patients will have more options available to them for treatment of a variety of chronic conditions,including treatment of type-2 diabetes.
read more
Disclosure forms provided by the author are available at NEJM.org.
Editor’s note:
Author Affiliations
Supplementary Material
| Disclosure Forms | 83KB |
Add your Comment

Add your Comment
Leave a Reply
You must be logged in to post a comment.
BHQJ 2018 ; 001:34-36
Related Article 
Medical Negligence & the Law5th May 2018 . Atrogenic harm is a matter of significant concern in Nigeria admin
Colorectal Cancer Overview5th May 2018 . [dkpdf-columns columns="3" equal-columns="false" gap="10"] Introduction Colorectal cancer is a major admin
Funding Healthcare Services in Nigeria – A conundrum of demand, policy and supply!5th May 2018 . [dkpdf-columns columns="3" equal-columns="false" gap="10"] Doctor, I happy say na you admin
5 “Provocations” of Healthcare Quality Reform6th May 2018 . [dkpdf-columns columns="3" equal-columns="false" gap="10"] n the four decades since he admin
Health Insurance, Activism & Urgent Change6th May 2018 . [dkpdf-columns columns="3" equal-columns="false" gap="10"] AR: Dr Soyinka, it’s wonderful to admin
Anne Olowu talks about her “Masterclass” experience6th May 2018 . [dkpdf-columns columns="3" equal-columns="false" gap="10"] As I suspect is the case admin
Stomach & Oesophageal Cancer in Nigeria6th May 2018 . [dkpdf-columns columns="3" equal-columns="false" gap="10"] Gastric and Oesophageal (Upper GI) cancers admin
Setting out the Stall!7th May 2018 . [dkpdf-columns columns="3" equal-columns="false" gap="10"] "The drawbacks of our false knowledge admin
Leave a Reply
You must be logged in to post a comment.